
Steps to Providing Quality Patient Care and Reducing Hospital Readmissions
There’s no doubt about it: In order to reduce hospital readmissions, hospitals have to place a stronger emphasis on quality patient care. But what exactly does this mean? Given that 50% of hospitals report that they fail to follow through on readmission reduction initiatives, it seems that this issue needs further clarification.
We recently reported on a study from Dartmouth that examined why hospital readmissions sometimes occur and concluded that the primary cause is “widespread and systematic failures in coordinating care for patients after they leave the hospital,” as it was phrased by the study’s principle investigator, Dr. David C. Goodman, M.D., M.S. Medicare penalties for high readmission rates continue to increase, and research firms everywhere are answering to the demands of more hospitals that are demanding explicit directives to reduce readmissions. Hundreds of studies are being produced in order to advise administrators on readmission reduction strategies, and the common factors all point to improving quality patient care. Here are some specific steps you can take to reduce hospital readmissions that we have found while compiling our own research:
- Form a Quality Improvement Team dedicated to reduce hospital readmissions. Just over half of hospitals report having a team working toward this goal. If your hospital is one that doesn’t, talk to a colleague in your area. Ask them to share their experiences with quality improvement teams and for advice on how to begin such an initiative.
- Increase the size of your nursing staff. Hospitals with more nurses are 25% less likely to be face Medicare readmission penalties than are hospitals with a smaller nursing staff. Nurses are the lynchpin for communication between patients and caretakers, and poor communication is one of the largest causes of hospital readmissions.
- Use NSQIP to collect readmission data. The fact that the Center for Medicare and Medicaid Services doesn’t have a standardized data tracking system for counting readmissions isn’t doing anyone any favors. The two major databases used for tracking readmissions–UHC and NSQIP–collect information in remarkably different ways and therefore produce remarkably different results. UHC collects its data from patient billing information. Using NSQIP requires nurses and other staff to manually enter information into the database. Although far more laborious than UHC, the higher level of human engagement involved in using NSQIP promotes better, more accurate data input. Dr. Elizabeth Wick of John Hopkins University explains, “Internally, if you want to improve patient care, it’s not enough just to know that the patient came back…You need to know why. And NSQIP data is key to providing those answers.”
- Establish an effective communication with external practitioners. Good communication is essential to the reduction of hospital readmissions. Always obtain the direct phone numbers of all patient caretakers and keep them for your own records. Provide copies of this contact information to patients as well as each medical practitioner on the contact list. Have this completed 48 hours prior to discharge in order to prevent any last-minute miscommunications during the stressful time of patient transfer.
- Empower patients by engaging them in the decision-making processes. Hospital staff—usually nurses—should establish a routine conversation to engage patients in discussions about their post-discharge care. When patients are given a sense of agency in their care they feel more empowered and are more likely to stick to their treatment plan. Have conversations about the responsibilities the patient must take for their own care, and also about what he or she needs to expect from others. If there are multiple treatment options, make sure to fully inform patients of the choices they have in treatment. All post-discharge plans for individual patients should be customized for that patient as much as possible.
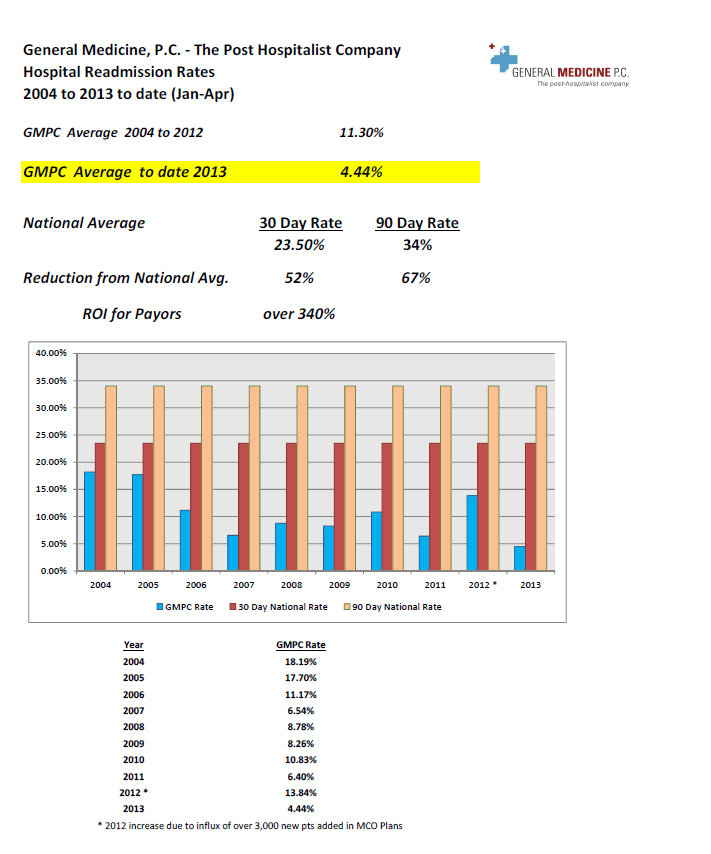
All of these efforts are noble attempts to reduce hospital readmission rates. Partnering with an external team of post-hospitalist specialists in addition to addressing internal systemic problems is also advised. For example, hospitals that integrated post-hospitalist services from General Medicine reduced readmissions by 52% from the national average. If you are interested in improving patient care and reducing hospital readmissions by integrating post-hospitalist specialists, find out more about ways you can partner with General Medicine.
{kind=link}

- How Post-Hospitalists Decrease Health Care Spending - 06-24-2015
- Top Reasons for Hospital Readmissions from SNFs - 06-03-2015
- The Real Cost of Hospital Readmission Rates - 05-20-2015